That hated hump!
In a person with scoliosis, forward bending of the trunk will cause a protuberance to appear on their back, at the level of the scoliotic curve: this anomaly is commonly referred to as a hump.
Scoliosis alters the alignment of the spine, and this alteration can be seen in the three dimensions of space: the affected vertebrae move sideways, taking on a different shape when viewed from the side; they also rotate, and this, especially if they are dorsal vertebrae, also causes a rotation of the rib cage.
This hump is an aesthetic problem for people with scoliosis, as they fear that it is obvious to everyone else. But that is not the case at all. There is often a world of difference between the problem itself and how it appears in everyday life.
During a thorough postural analysis or a medical examination, the doctor or examiner will position the patient’s body to emphasise any asymmetries present precisely so that they can be identified and measured.
Nobody is perfectly symmetrical in daily life: when we move, we frequently twist our bodies and bend and rotate our joints, our movements involving different segments of our body in various combinations. As a result, we constantly develop asymmetries, humps, and combinations of bent and straight segments without even being aware of it.
Let’s take an example. A doctor examining a patient’s hump will have the youngster stand with his knees straight and body bent forwards so as to emphasise the protuberance on the side of the curve. Is it visible? Yes, if the patient’s scoliosis is sufficiently marked, it will be visible even to the untrained eye.
Now, what if we ask someone with a healthy back to tie up their shoelace? To do this, most people will push their foot forward, bend their knees asymmetrically, and lean forwards, with their trunk deviating to one side (the side of the shoe needing to be tied). As they do this, their spine will be turned to one side, and a hump can be seen on their back, on the side of the leg, with the shoe needing to be tied. Does that hump mean they have scoliosis? Of course not! It is caused by them twisting their spine in order to reach their shoe.
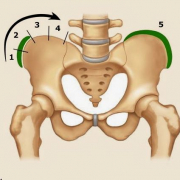
We can explain the scoliosis-induced asymmetry of the hips in a similar way. If we stand still with our feet parallel, our knees straight and our trunk aligned, our side and our hips will look symmetrical; in people with scoliosis, on the other hand, one hip will appear straighter in respect to the other.
Now, let’s imagine how we normally stand. Do we ever actually stand with our feet positioned symmetrically and our bodyweight perfectly distributed between them? No! We usually stand with our weight on one foot and one hip thrust out. How do we look in this position? It is completely asymmetrical, but this asymmetrical appearance is due to our natural posture; it is not caused by scoliosis!
Nobody ever notices these natural asymmetries because our bodies repeatedly assume them throughout the day. For this reason, even asymmetries caused by scoliosis are never really noticed by others.
Going back to our “hump”: is it really such a bad thing, to the point that we should do everything in our power to get rid of it?
The back brace sometimes worn by youngsters with scoliosis, seeks to optimise the alignment of the vertebrae involved in the scoliosis curve, but how? It works by pushing “from the outside” directly on the affected portion to restore its symmetry. The force it exerts on the rib cage or on the soft tissues of the hips also affects the spine.
What is meant by an optimal alignment of the spine? The straightest possible?
This isn’t an easy question to answer. Equally, it is not easy for the doctor to identify the correct balance of forces to be exerted on the spine by the brace pads.
The best alignment will enable the treated spine to remain as stable as possible and to withstand the forces to which it is subjected in daily life.
The strength of the spine depends to a large extent on its shape, as seen from the side. From this perspective, our spine is characterized by two curves, called lordosis and kyphosis. These curves must be well balanced: neither too pronounced nor too slight.
Unfortunately, in scoliosis, and this applies particularly to dorsal scoliosis, the kyphotic curve is reduced, causing the back to appear flat or even hollow. In other words, the normal direction of spinal curvature is reversed, and the spine is weaker as a result.
Unfortunately, the brace has no way of counteracting this problem, as all it can do is push. In fact, its corrective forces, which are applied to the hump to help align the vertebrae involved in the curve, have a flattening effect on the back’s upper part (dorsal section).
Therefore, the doctor’s task is to find and maintain the best possible balance, considering the importance of all the planes of the spine.
What this means in practice is that it is sometimes necessary not to “go too far” in trying to eliminate the hump. Because if this objective can be achieved only by excessively reducing the dorsal kyphosis angle, the result will be a weaker and less healthy spine.