Modular Italian Brace works just as well as the Sforzesco
A modular brace that has the same practicality and comfort of wearing and the same proven effectiveness, even on the most severe curves, of the Sforzesco corset but with significantly reduced costs. It is the Modular Italian Brace (MIB), the latest corset developed by our institute, after the Sforzesco and the Sforzesco Free Plevis.
Its effectiveness is demonstrated by the data of one of our studies recently published in the Journal of Clinical Medicine, The New Modular Sforzesco Brace (Modular Italian Brace) Is as Effective as the Classical One: A Retrospective Controlled Study from a Prospective Cohort. “A research of considerable importance,” comments Dr. Francesco Negrini, physiatrist and author of the study. “We recently developed a new Sforzesco brace based on modularity (the Modular Italian Brace—MI brace) that could allow standardisation, facilitating global expertise diffusion, increased modifiability and adaptability, and cost savings due to longer brace life”.
We remind you that the Sforzesco brace is a very rigid push-up brace effective in adolescent idiopathic scoliosis (AIS), which revolutionised rehabilitation treatment years ago by replacing the cast but guaranteeing the same results. Recently, the “Free Pelvis” (FP) innovation has been introduced. It consists of semi-rigid material on the pelvis connected to the main rigid body of the brace on the trunk.
It was found that it does not change the in-brace and short-term results of classical very rigid braces and, consequently, can be safely applied.
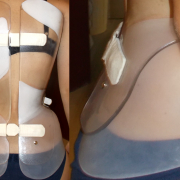
The MI brace, even if built in a different way, keeps the main characteristic of the Sf brace, that is, the overall symmetry (with some asymmetries inserted in specific areas). In fact, it is the symmetry that allowed the development of the MI brace, where it is possible to recreate the asymmetrical needs of the SF brace through internal pads.
The MIB can be built and fully personalised directly for the patient, modifying the classical procedures of brace construction through CAD-CAM or casting. Moreover, the MIB can be continuously adapted during treatment, giving full adaptability to the patient during changes due to growth or treatment.
The MIB is an evolution of the SF-FP. The two braces share the semi-rigid material on the pelvis, a novelty that improves comfort and patient acceptability. On the other hand, Sf FP is built in a more traditional way, without the MIB modularity and the possibility to adapt the brace during treatment. With Sf FP, if the patient changes due to growth, the brace must be changed altogether.
“The braces considered in this paper share the same action; the question is if they also share the same results. We aimed to compare the short-term results of the two braces,” explains Dr. Negrini. “We compared in this retrospective study 231 patients with scoliosis, between 10 and 16 years old, 53 treated with a MI brace, and 178 treated with a Sforzesco brace. Both braces reduced the Cobb angle (−6◦ out-of-brace; −16◦ in-brace) without differences between groups. The results of the present study suggest that the SfB and MIB can have similar positive short-term results on moderate-to-moderate, moderate-to-severe, and severe curve brace treatment with modular braces. that could lead to easier diffusion worldwide, even where there are reduced economic means and expertise in brace treatment. Before suggesting a generalised use of the MIB as a first-line rigid brace treatment, the results should be confirmed in studies with longer follow-ups”.